Sep 25, 2024
Written by Toby Emanuel, MD, Director of Life Science Innovation at Viz.ai

Lung diseases–including lung cancer, chronic obstructive pulmonary disease (COPD), asthma, pulmonary arterial hypertension (PAH), interstitial lung disease (ILD), and bronchiectasis–impact millions globally and rank among the top causes of morbidity and mortality.1 Despite significant advances in treatment, many patients continue to face diagnostic delays, fragmented access to specialty care, and underutilization of guideline-directed therapies.
At Viz.ai, we have demonstrated that AI-powered software has the potential to address these gaps. Our pulmonary embolism solution, Viz PE, was associated with a 98% reduction in time to assessment and a 74% decrease in in-hospital mortality for pulmonary embolism.2 We’ve also demonstrated AI’s ability to accelerate diagnosis and support adherence to guideline-directed care. For example, in hypertrophic cardiomyopathy (HCM), Viz HCM helped patients reach a diagnosis in three months has reduced the time to diagnosis to 3 months vs. the standard of care of ≤ 2 years.3 In post-acute stroke, we’ve seen Viz.ai increase identification of patients receiving guideline-aligned care by 8x compared to standard workflows.4,5
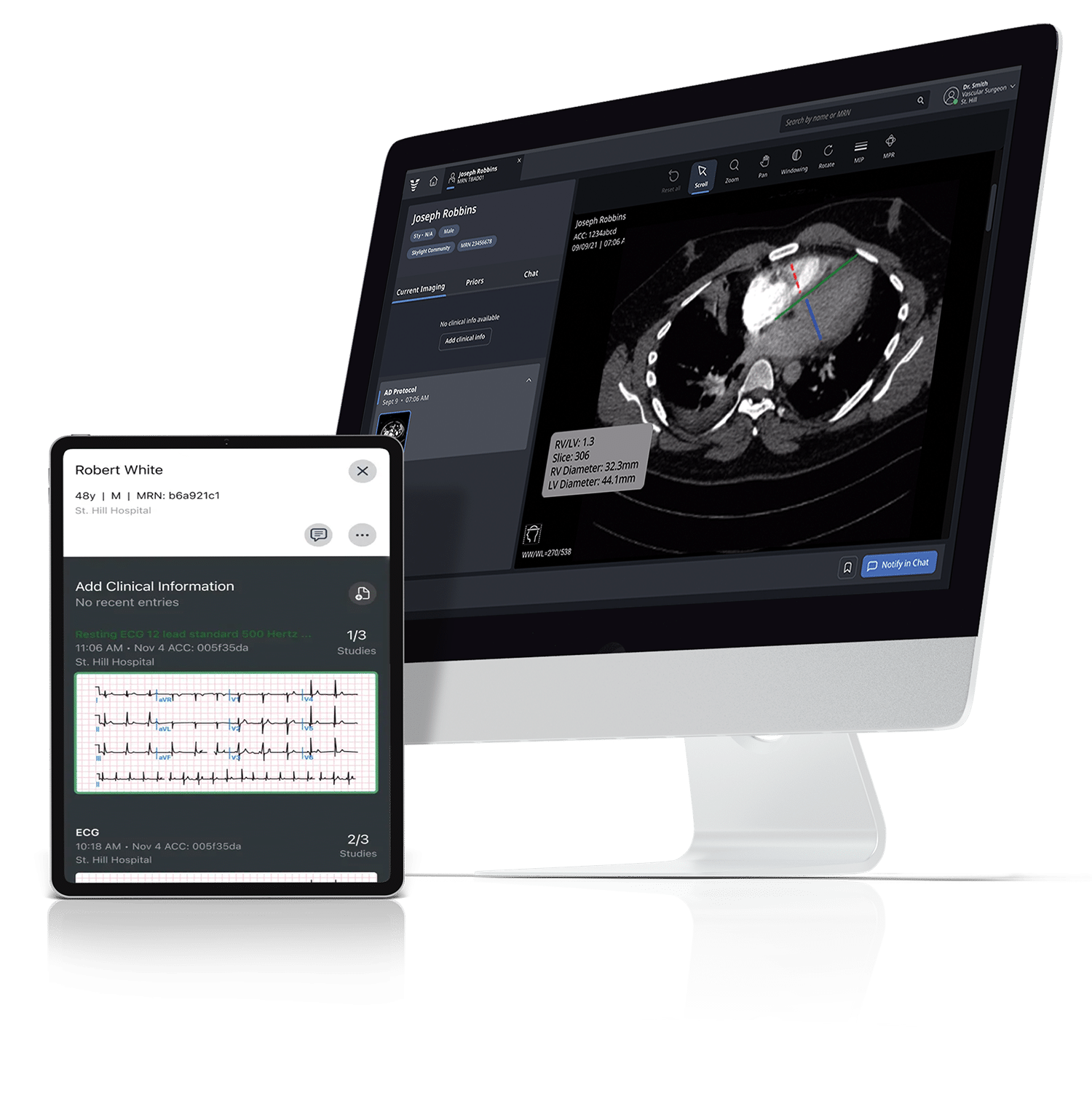
These solutions are built to fit within existing clinical workflows, helping care teams quickly access and act on the most relevant patient information. By streamlining how insights are surfaced and shared, Viz.ai supports more timely, coordinated decision-making—while keeping clinical judgment and treatment decisions firmly in the hands of the treating provider.
The impact that AI-powered care coordination software can have on patient care is becoming increasingly evident. Below, I’ve highlighted three ways in which we see technology continuing to drive better care in lung disease.
Diseases like lung cancer, pulmonary hypertension, and interstitial lung disease can present with subtle, non-specific findings that make diagnosis challenging. Other times, diseases are identified through incidental findings, like a lung nodule found on an unrelated imaging scan. In one study, only 36% of patients with lung nodules received any subsequent workup.6 We can and must do better.

Bronchiectasis is another example of this gap. Despite affecting an estimated 500,000 to 600,000 adults in the U.S., the condition remains among the most underdiagnosed chronic lung diseases.7 Its cardinal symptoms–chronic productive cough, recurrent infections, and dyspnea–overlap substantially with COPD, asthma, and chronic bronchitis, resulting in frequent misclassification. Published data suggest patients wait up to 10 years or more from symptom onset to confirmed diagnosis.7,8 Bronchiectasis is definitively diagnosed by High-Resolution CT, yet many at-risk patients never receive imaging in the first place.9 AI can help by flagging EHR signals that suggest undiagnosed bronchiectasis risk and surfacing incidental CT findings that were never followed up clinically.

AI has vast potential to enhance diagnostic accuracy and detect or even predict disease; however, some of the most successful use cases we see tend to be centered around addressing existing gaps in care. A major theme we see across health systems today is administrative burden and lack of capacity, so solutions that act as triage tools, a second set of eyes, or automate manual processes can be some of the most impactful.
For example, an AI algorithm can help automatically identify a patient with a pulmonary nodule that was lost to follow-up or prompt a physician to take a closer look at subtle findings suggestive of ILD. These types of algorithms can be quite impactful when paired with thoughtful integration into provider workflows.
For chronic conditions like COPD and asthma, patients can present with exacerbations to outside emergency departments or urgent care facilities, making it difficult to follow their care over time. This can lead to repeat exacerbations, hospital readmissions, and delays in therapy optimization. Notably, COPD has one of the highest 30-day readmission rates, comparable to conditions like pneumonia and heart failure.10
Bronchiectasis presents a similar coordination challenge. Patients frequently cycle through primary care and emergency departments for recurring respiratory infections, often receiving steroids and antibiotics for presumed COPD or asthma exacerbations rather than bronchiectasis-directed care.11 Because exacerbations are independently associated with faster lung function decline, the cost of this misrouting compounds over time.12 Care coordination tools that can aggregate clinical history and exacerbation history across care settings, generate care coordination prompts with relevant clinical context, and help reduce missed post-discharge follow-up can materially close these gaps.
Digital care coordination tools can help bridge some of these gaps by creating virtual “hubs” that flag high-risk patients, pull together information from disparate sources, summarize the information most relevant to a specific provider (e.g., a pulmonologist or oncologist), and enable cross-specialty HIPAA-compliant communication. When specialists have limited capacity and a mere 15 minutes per patient, AI-powered tools that help generate a quick and comprehensive understanding of a patient’s care since their last visit and streamline next steps can be invaluable. EHR systems are not designed for this coordination but as systems for transaction tracking, billing, and audit trails.
Given AI’s vast potential at the point of care, it’s no surprise that three in five health systems are integrating AI into care delivery,13 and 88% of healthcare leaders are already reporting significant improvements, including faster diagnoses, better care coordination, and more efficient workflows.14

Advances in precision medicine have ushered in new, targeted therapies for diseases like non-small cell lung cancer (NSCLC) that have led to remarkable improvements in outcomes but also introduce additional complexity to care delivery. While specialized thoracic oncologists may be able to focus their time and attention on digesting the latest evidence in lung cancer, up to 80% of patients are treated by community oncologists who treat a wide variety of cancer types.15 For community oncologists, keeping up with rapidly advancing guidelines and evidence for lung, breast, prostate, GI, and hematologic cancers can be daunting.
A similar dynamic is emerging in bronchiectasis. New treatments approved by the FDA are reducing exacerbation rates by targeting the neutrophil-driven inflammatory cycle.16 But many patients who may meet clinical criteria, including based on exacerbation history, are not always recognized or evaluated in a timely manner.7,17 AI that can align patient data with relevant clinical guidelines at the point of care may help clinicians identify appropriate next steps for evaluation and management.
Building on the concept of virtual “hubs” that help highlight high-risk patients and summarize relevant information, AI can play a crucial role in ensuring patient-specific, contextualized information about the latest guidelines and evidence-based practices is delivered to providers who need it. For instance, AI could review a patient’s medical record and cross-reference it with NCCN guidelines to surface clinically relevant, guideline-based information for clinician consideration, including potential treatment options or even relevant clinical trials.

AI-powered digital care coordination has the potential to transform lung disease management and more. By facilitating early detection, improving care continuity, and supporting more personalized, evidence-based care, these tools can unlock a future where patients receive more timely, comprehensive care. For clinicians, AI can reduce the burden of information overload, bringing critical insights to the surface and enhancing the ability to make well-informed decisions.
We’re excited to continue building out this future together so we can reshape patient care to improve outcomes and, ultimately, save lives.

Examples below highlight collaborations focused on workflow efficiency and care coordination.
Sep 25, 2024

New software will incorporate natural language processing (NLP) for more effective patient screening and follow-up SAN FRANCISCO – October 21,...
Oct 21, 2024
New partnership brings together AI experts and lung cancer researchers to improve early disease detection SAN FRANCISCO – September 4,...
Sep 04, 2024
New partnership to identify and quantify lung nodules SAN FRANCISCO – April 10, 2024 – Viz.ai, the leader in AI-powered...
Apr 10, 2024
Company’s Artificial Intelligence Technology Shows Better Results in Early Detection and Patient Care SAN FRANCISCO, CA – September 21 –...
Sep 21, 2023
Company’s artificial intelligence technology shows 74% reduction in in-hospital mortality rates for pulmonary embolism SAN FRANCISCO – March 7, 2024...
Mar 07, 2024
Viz Life Sciences
In partnership with pharmaceutical and medical device companies, Viz.ai develops new, customized solutions for treatable decisions.
Learn more