Viz™ CTP
A comparison of two automated CTP algorithms for estimation...
Background Automated analysis of CT perfusion data has become an integral part of stroke triage. Many vendors calculate cerebral blood...
Jul 26, 2021
Automated analysis of CT perfusion data has become an integral part of stroke triage. Many vendors calculate cerebral blood flow (rCBF) and time to maximum perfusion (Tmax) in attempts to estimate core infarct, reported as rCBF<30%, versus tissue at risk, reported as Tmax>6 seconds. We compare the algorithms of two widely available software platforms, iSchemaView Rapid and Viz.AI.
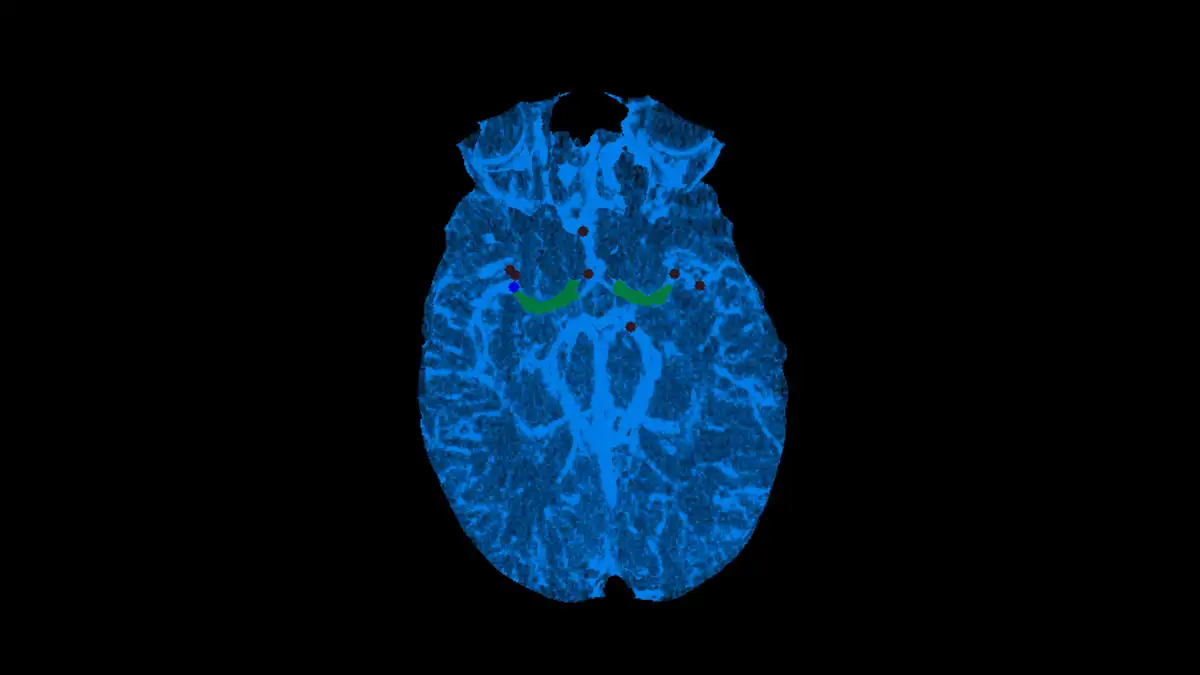
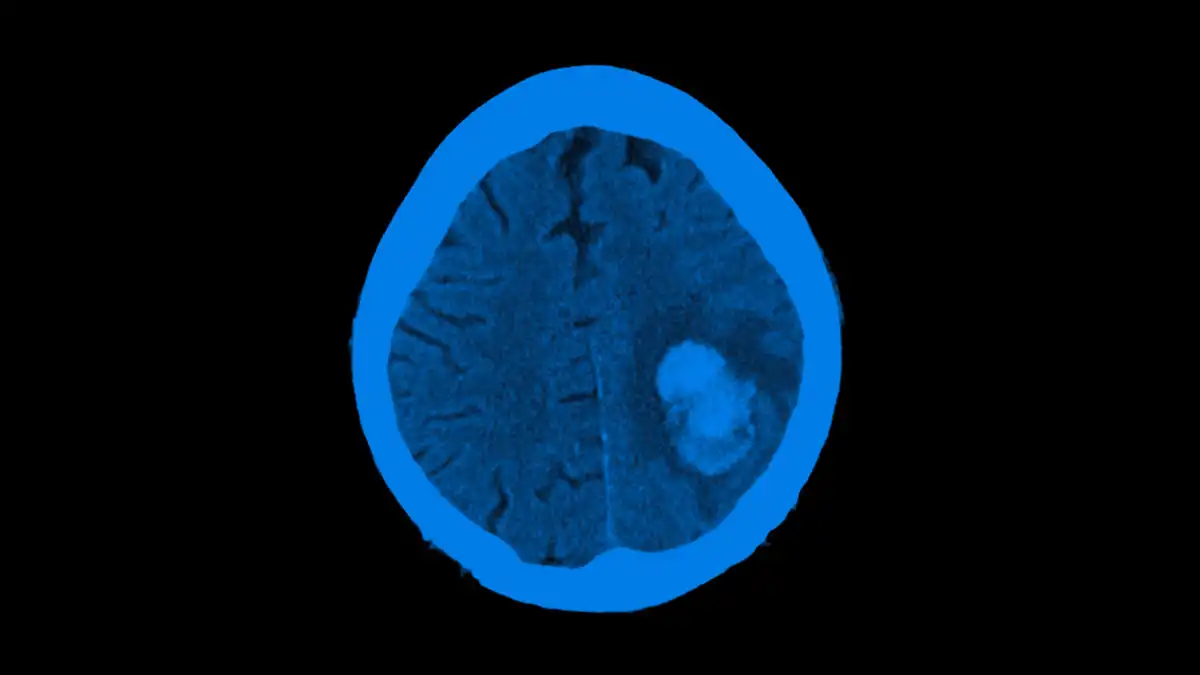
All patients on whom CT perfusion imaging for the suspicion of acute ischemic stroke was performed and also had subsequent underwent MRI imaging within 24 hours of CTP were included. As, sme patients underwent mechanical thrombectomy, rCBF<30% volumes were calculated to restrict analysis to core infarct. Both iSchemaView Rapid and Viz.AI software platforms were concurrently used. Final infarct volume was estimated off the B1000 sequence, in which areas of high signal were manually segmented using Slicer 3D.
26 patients were identified. 14 underwent mechanical thrombectomy (53.8%), of which 13 were recanalized to TICI 2C or better (92.9%). rCBF<30% volumes calculated by both RAPID and Viz were to the segmented final infarct volume on MRI. The average differences was 30.73 (+/- 38.7) cc for RAPID and 23.05 (+/- 39.7) cc for Viz, which was not significantly different (p=0.515).
There was not a statistically significant difference in calculated rCBF<30% volumes between Viz or Rapid, compared to the manually segmented volumes from the 24 hour diffusion MRI.
Researcher:
Jan Vargas , MD
Publication:
Journal of NeuroInterventional SurgeryDate Published: July 26, 2021
Jul 26, 2021
Viz™ CTP
Background Automated analysis of CT perfusion data has become an integral part of stroke triage. Many vendors calculate cerebral blood...
Jul 26, 2021
Viz™ AORTIC
Background After years of both increasing enthusiasm and skepticism by surgeons and patients, the first artificial intelligence (AI) and machine...
May 05, 2023
Viz™ LVO
Background Artificial intelligence (AI) software is increasingly applied in stroke diagnostics. However, the actual performance of AI tools for identifying...
Jan 27, 2022